
Júlio Leal Villela Garcia, Vanessa Rodrigues do Prado Garcia, Sandro Marcelo de Moraes Valente
Resumo
Introdução: No contexto da lipoescultura, a lipoaspiração cervicofacial envolve a aplicação de pressão negativa por meio de uma cânula oca no plano subcutâneo para remover suavemente células de gordura e esculpir com precisão depósitos indesejados de gordura no rosto e pescoço. Além disso, o contorno lipo oferece uma ferramenta versátil no arsenal do cirurgião facial para alcançar o perfil facial desejado. Em 2020, aproximadamente 15,5 milhões de procedimentos estéticos foram realizados somente nos Estados Unidos.
Objetivo: Foi realizada uma revisão sistemática sobre os principais resultados clínicos, apresentando estudos sobre o risco de viés e os avanços na lipoescultura facial e cervical como uma importante ferramenta estética para o cirurgião-dentista.
Métodos: Foram seguidas as regras da Plataforma PRISMA de Revisão Sistemática. A busca foi realizada de novembro de 2021 a fevereiro de 2022 nas bases de dados Scopus, PubMed, Science Direct, Scielo e Google Scholar.
Resultados: Foram encontrados 64 artigos envolvendo lipoescultura. Um total de 32 artigos foi totalmente avaliado e 14 foram incluídos e desenvolvidos no presente estudo. Considerando a ferramenta Cochrane para risco de viés, a avaliação geral não resultou em estudos com risco significativo de viés. O gráfico Funnel Plot apresentou comportamento simétrico. Vinte e cinco estudos não atenderam aos critérios do GRADE. A maioria dos pacientes envolvidos nos estudos demonstrou melhorias no aumento e contorno facial. Em pacientes com perda de volume facial, a transferência de gordura de alta densidade com injeção facial de gel SVF resultou em escores de melhora significativamente mais altos e melhor satisfação do paciente.
Conclusão: De acordo com os principais estudos clínicos selecionados no presente estudo, a lipoescultura cervicofacial demonstrou ser segura e eficaz. Em pacientes com perda de volume facial, a transferência de gordura de alta densidade com injeção facial de gel SVF resultou em escores de melhora significativamente mais altos e melhor satisfação do paciente. Ainda assim, os resultados dos estudos mostraram que o nível de autoconfiança e a qualidade de vida relacionada à saúde mental podem ser significativamente melhorados após o tratamento de preenchimento facial com gordura.
Palavras-chave: Lipoescultura. Enxerto de gordura. Contorno lipo. Lipoescultura facial. Lipoescultura cervical. Estética. Ensaios clínicos.
Introdução
No contexto da lipoescultura, a lipoaspiração cervicofacial envolve a aplicação de pressão negativa por meio de uma cânula oca no plano subcutâneo para remover suavemente células de gordura e esculpir com precisão depósitos indesejados de gordura no rosto e pescoço. Além disso, o contorno lipo fornece uma ferramenta versátil no arsenal do cirurgião facial para alcançar o perfil facial desejado [1–3]. Em 2020, aproximadamente 15,5 milhões de procedimentos estéticos foram realizados nos Estados Unidos. Técnicas minimamente invasivas que permitem uma recuperação mais rápida estão especialmente em demanda. Segundo o relatório de 2018 da The Aesthetic Society, a lipoaspiração é o segundo procedimento estético mais popular nos Estados Unidos [1].
Nas últimas décadas, também foram observadas melhorias nas técnicas de suspensão do sistema músculo-aponeurótico superficial e dos coxins de gordura adjacentes. Assim, a lipoescultura (LS) pode complementar a cirurgia de envelhecimento cervicofacial [2,3]. Procedimentos minimamente invasivos em lipoescultura facial estão se expandindo, e a transferência de tecido adiposo pode resultar em efeitos estéticos ideais [3–5].
As técnicas atuais de lipoaspiração evoluíram ao longo dos anos. Inicialmente, fazia-se a excisão direta de coxins de gordura inestéticos, descrita em combinação com lifting do sistema músculo-aponeurótico superficial (SMAS). A gordura pode ser removida por incisões de ritidectomia submentonianas e pós-auriculares, ou o excesso de gordura ptótica e pele pode ser excisado diretamente das bochechas e do queixo duplo. No entanto, como é tecnicamente desafiador remover uniformemente os depósitos de gordura subcutânea com técnicas abertas, essas tentativas frequentemente resultam em contornos de pele irregulares.
Nesse sentido, as técnicas de contorno lipo fornecem um meio de modelar os depósitos de gordura no pescoço e rosto para alcançar melhor o perfil facial desejado [6]. A melhoria geral resultante tem efeitos diretos e indiretos na estética facial. Por exemplo, a lipoaspiração submentoniana produz um ângulo cervicomentoniano mais agudo e agradável e, ao mesmo tempo, dá a ilusão de maior projeção do queixo [7].
Historicamente, a excisão direta da pele e da gordura levava a cicatrizes longas e visíveis que eram propensas à depressão central e formação de “orelhas de cachorro” no pós-operatório. Diante dos resultados frequentemente insatisfatórios com a excisão direta da gordura, não era incomum que cirurgiões ignorassem os acúmulos de gordura pré-auricular, nasolabial, submentoniana e cervical, muitas vezes produzindo uma discrepância marcada entre a aparência rejuvenescida da parte superior do rosto em comparação com a parte inferior e o pescoço [8].
Nas últimas décadas, a introdução de técnicas refinadas de lipoaspiração, além da plicatura do platisma e do tensionamento cirúrgico da pele excedente do pescoço, deu ao cirurgião plástico facial a capacidade de melhorar o contorno da mandíbula e a definição do ângulo cervicomentoniano. A versatilidade do procedimento de lipoescultura, usado isoladamente ou em combinação com ritidectomia, implantes malares e de queixo, mentoplastia e outros procedimentos adjuvantes da cirurgia plástica facial, combinada com seus excelentes resultados, cicatrizes pequenas e discretas, facilidade técnica e mínima morbidade e recuperação, popularizou seu uso [7].
Dessa forma, cirurgiões-dentistas começaram a aplicar esses princípios ao pescoço e à região mandibular para rejuvenescimento facial por meio de incisões de acesso mínimo, incluindo lipectomia ultrassonográfica endoscópica e o uso de liposhavers. A lipoescultura facial se concentra no reposicionamento do tecido adiposo e no aumento das zonas de transição facial. Isso é feito utilizando suturas internas de suspensão, bem como enxerto autólogo de gordura [6]. Assim, a LS é uma alternativa ao rejuvenescimento facial que envolve a pele, liberação dos ligamentos de sustentação e remoção adequada do tecido adiposo da camada subcutânea, ao mesmo tempo que melhora o tônus da pele e o contorno facial.
Um estudo também apresentou experiências com 312 pacientes submetidos a rejuvenescimento cervicofacial, demonstrando os benefícios da lipoescultura nesse contexto: redução de rugas do tipo “marionete”, remoção de acúmulos periorais, contorno facial em “V”, definição da mandíbula, redução de papada, projeção do queixo e elevação cervicofacial [7]. Assim, a lipoaspiração foi um divisor de águas na evolução da lipoescultura cervicofacial, permitindo a remoção permanente do excesso de tecido adiposo localizado sob a pele. Além disso, vários recursos terapêuticos estão em constante aperfeiçoamento, como o uso de cânula cortante seguida de cânula romba, lipoaspiração assistida por laser/ultrassom, bem como cânulas rotativas e vibratórias [8].
Métodos
Desenho do Estudo
Foram seguidas as regras da Plataforma PRISMA para Revisão Sistemática (Relato transparente de revisões sistemáticas e meta-análises – http://www.prisma-statement.org/).
Fontes de Dados e Estratégia de Pesquisa
As estratégias de busca para esta revisão sistemática foram baseadas nos termos de busca (MeSH Terms):
“Liposculpture. Fat grafting. Lipocontour. Liposculpture face. Cervical liposculpture. Aesthetics. Clinical trials”.
A busca foi realizada de novembro de 2021 a março de 2022 nas bases de dados Scopus, PubMed, Science Direct, Scielo e Google Scholar. Além disso, foi utilizada uma combinação de palavras-chave com os operadores booleanos “OR”, “AND” e “NOT” para direcionar artigos científicos de interesse.
Qualidade dos Estudos e Risco de Viés
A qualidade dos estudos foi baseada no instrumento GRADE [9] e o risco de viés foi analisado segundo a ferramenta Cochrane [10].
Resultados e discussão
Resumo dos achados
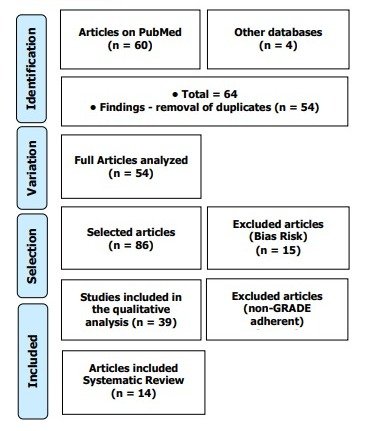
Foram encontrados 64 artigos envolvendo lipoescultura facial e cervical. Inicialmente, foram excluídas duplicações de artigos. Após esse processo, os resumos foram avaliados e uma nova exclusão foi realizada, removendo os artigos que não abordavam o tema deste estudo. Um total de 32 artigos foi avaliado integralmente e 14 estudos clínicos foram incluídos e desenvolvidos na revisão sistemática. Vinte e cinco estudos não atenderam aos critérios do GRADE (Figura 1). Considerando a ferramenta Cochrane para risco de viés, a avaliação geral não resultou em estudos com risco significativo de viés (Figura 2).
Figura 1. Seleção de artigos (Revisão Sistemática, N=14 estudos clínicos).
A Figura 2 apresenta os resultados do risco de viés nos estudos utilizando o gráfico Funnel Plot, por meio do cálculo do Tamanho do Efeito (Teste de Cohen). O tamanho da amostra foi determinado indiretamente pelo inverso do erro padrão (1/Erro Padrão). O gráfico apresentou comportamento simétrico, não sugerindo risco significativo de viés nos estudos com tamanhos amostrais pequenos que estão representados na parte inferior do gráfico.
Figura 2. O gráfico Funnel Plot simétrico não sugere risco de viés entre os estudos com pequeno tamanho amostral que estão representados na parte inferior do gráfico.
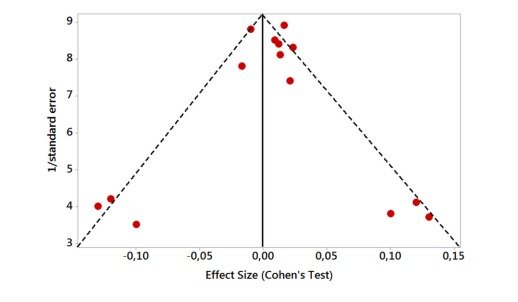
Figura 3 apresenta três imagens ilustrativas, onde as imagens A e B representam o posicionamento e a penetração da cânula para lipoaspiração, e a imagem C representa o resultado da redução do tecido adiposo na região destacada. As imagens pertencem a uma paciente (com informações confidenciais, sem apresentação do caso clínico) dos autores do presente estudo, com o objetivo de exemplificar o procedimento de lipoescultura, bem como demonstrar que o procedimento pode ser realizado com segurança.
Aspectos Genéticos, Epigenéticos e Fisiopatológicos como Preditores para Lipoescultura
As características cervicofaciais de cada indivíduo são determinadas pela estrutura óssea e cartilaginosa subjacente, e pela cobertura da pele e do envelope de tecido mole. Essas características são todas determinadas em nível genético, mas podem ser influenciadas em diferentes graus por fatores ambientais (epigenéticos), como nutrição, exercícios, envelhecimento, medicamentos, exposição a toxinas, danos actínicos, traumas e cirurgias [11,12].
À medida que os fatores epigenéticos adversos exercem seu impacto, ocorre a ptose das estruturas de sustentação facial, o que leva à queda dos coxins de gordura malares e bucais. A perda da elasticidade da pele produz rugas grossas e finas, além da flacidez da pele facial. A frouxidão dos tecidos e a má distribuição dos depósitos de gordura levam à formação de papada e queixo duplo, com tecidos soltos e redundantes pendendo sobre a mandíbula e o queixo, respectivamente. No pescoço, o acúmulo de gordura e a ptose do platisma resultam em bandas proeminentes, produzindo uma aparência de “pescoço de peru”. Pacientes com ossos hióides congênita e anatomicamente baixos apresentam uma definição mais comprometida do ângulo cervicomentoniano [12].
Figura 3. Três imagens ilustrativas, onde as imagens A e B representam o posicionamento e a penetração da cânula para lipoaspiração, e a imagem C representa o resultado da redução do tecido adiposo na região destacada.
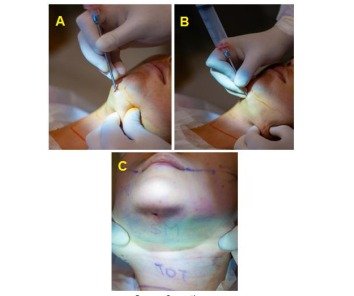
Source: Own author
Além disso, a perda de gordura facial foi enfatizada como um componente do envelhecimento [12-14]. A redução de volume, particularmente nas áreas periorbitais, bochechas e periorais, desempenha um papel proeminente na criação de cavidades faciais e flacidez da pele. A remoção de gordura corporal de determinados locais e a subsequente reinjeção em áreas de atrofia é o ideal [15-18]. A viabilidade da gordura é influenciada por diversos fatores, incluindo o método de coleta, limpeza, tamanho das partículas e tamanho da cânula de reinjeção. Minimizar a pressão de extração a vácuo causa menos trauma celular imediato. As menores cânulas devem corresponder à cânula de injeção para minimizar a compressão durante a transferência. A limpeza pode ser realizada por lavagem ou centrifugação. Recomenda-se o uso de pedaços menores de tecido adiposo para minimizar nódulos e aumentar a área de superfície [19].
Nesse contexto, é importante observar que as áreas mais comuns de injeção de gordura são as bochechas e os sulcos nasolabiais, onde o tecido é mais espesso e os movimentos musculares são mínimos. As injeções periorbitais são outra opção, mas partículas muito finas são necessárias para evitar a formação de nódulos. A área perioral e os lábios são os menos previsíveis quanto à retenção, presumivelmente devido ao movimento muscular subjacente [7].
Além disso, alguns indivíduos jovens têm uma propensão genética à distribuição indesejável de gordura facial, apesar do peso corporal normal. Por exemplo, o acúmulo submentoniano de gordura em bebês pode persistir na vida adulta. Esses pacientes geralmente apresentam excelente tônus de pele e muscular e podem se beneficiar apenas de uma lipoaspiração seletiva e fechada. O acúmulo de gordura na idade adulta pode ocorrer devido à hiperplasia de adipócitos e não à divisão celular. A lipoaspiração reduz o número total de adipócitos ao remover diretamente as células e induzir apoptose localizada como resultado de trauma mecânico e desvascularização. Os adipócitos que permanecem após a LS são uma população estável e não são mais propensos à hiperplasia do que os adipócitos de outras partes do corpo. Assim, a melhora do perfil facial após a lipoaspiração é mantida enquanto não houver um ganho de peso excessivo generalizado [3].
Cuidados Pós-operatórios Principais
O manejo pós-operatório é dividido em período pós-operatório imediato (as primeiras 24 horas) e o período subsequente. O cuidado pós-operatório imediato foca na prevenção de hematoma por meio do controle da pressão arterial. Novamente, para fins práticos, o nível da pressão arterial sistólica é mais indicativo do que o da diastólica. A manutenção de uma pressão sistólica pós-operatória inferior a 140 mmHg é desejável [20].
O tratamento intraoperatório com um adesivo transdérmico de clonidina de 0,1 a 0,2 mg frequentemente atenua a hipertensão associada à injeção e, subsequentemente, a absorção de epinefrina da solução anestésica local. Em pacientes que não utilizam medicação para pressão arterial (particularmente betabloqueadores), a hipertensão intraoperatória pode ser controlada com bolus de labetalol de 5 a 10 mg. É importante evitar adicionar betabloqueadores em pacientes que já estão sob efeito de betabloqueio e apresentam bradicardia relativa. Nesses pacientes, pode-se administrar um bolus intraoperatório de 0,25 mg de bloqueadores dos canais de cálcio, como a nicardipina.
A adrenalina injetada da solução anestésica local é absorvida lentamente, então as equimoses pós-operatórias geralmente ocorrem entre quatro e dez horas após a cirurgia. No pós-operatório, o labetalol pode ser administrado por via oral em doses de 100 mg. Alternativamente, um agonista alfa puro (como clonidina de 0,1 a 0,3 mg) pode ser administrado por via oral [21].
Além disso, o inchaço prolongado no pós-operatório pode causar estresse de relaxamento da pele facial e levar a um resultado comprometido. O grau de edema pós-operatório está relacionado à extensão da dissecção, não à profundidade. A ingestão limitada de sal (preferencialmente 1000 mg/dia) e a redução da ingestão de líquidos também podem ser benéficas. O valor potencial dos corticosteroides perioperatórios continua controverso. Enquanto cirurgiões craniomaxilofaciais consideraram seu uso benéfico, outros autores não encontraram benefício para o inchaço em ritidoplastias [20,21].
Complicações Principais [3]
✓ Hematoma
✓ Necrose cutânea
✓ Infecção
✓ Lesão nervosa
✓ Fibrose
✓ Deformidades (hipotrofia ou hipertrofia)
Principais Estudos Clínicos – Revisão Sistemática
Análise (N=14 estudos clínicos)
No contexto de lipoenxertia e lipoescultura, o tratamento para melhorar características da pele relacionadas ao envelhecimento, como rugas, manchas pigmentares, poros ou rosácea, tornou-se uma prática para melhorar a saúde da pele e do organismo como um todo, uma vez que isso impacta positivamente na qualidade de vida dos pacientes. Nesse sentido, estão sendo realizadas otimizações. Assim, diferentes aditivos como plasma rico em plaquetas (PRP) ou fração vascular estromal (SVF) têm sido combinados com a lipoenxertia para aumentar o efeito terapêutico e a estabilidade das células estromais derivadas do tecido adiposo (ASCs).
Para esse fim, um estudo randomizado, prospectivo, duplo-cego e controlado por placebo examinou a hipótese de que o SVF isolado mecanicamente potencializa o efeito terapêutico da lipoenxertia suplementada com PRP para melhorar a qualidade da pele facial. No total, 28 mulheres foram incluídas; 25 completaram os acompanhamentos dentro de 1 ano do pós-operatório. Comparado à lipoenxertia suplementada com PRP, a lipoenxertia suplementada com PRP combinada com SVF não melhorou a qualidade da pele facial nem a satisfação das pacientes em uma população saudável, mas foi um procedimento seguro [22].
Além disso, um estudo investigou o impacto de uma intervenção estética na autopercepção de melhora na aparência facial e na qualidade de vida (QoL) após 1 e 6 meses de acompanhamento. Um total de 63 indivíduos consecutivos submetidos à lipoenxertia facial foram incluídos no estudo. Houve uma melhora estatisticamente significativa na qualidade de vida em cada ponto subsequente, em comparação à linha de base, em todos os domínios do SF-36, exceto nas subescalas de funcionalidade física e dor. É notável que a vida social ativa esteve fortemente associada à maior satisfação com a aparência facial, melhor autoestima e menores níveis de ansiedade e depressão durante o período de acompanhamento após a lipoenxertia facial. Os resultados deste estudo apoiam a hipótese de que o nível de autoconfiança e a qualidade de vida relacionada à saúde mental podem ser significativamente melhorados após o tratamento com lipoenxertia facial [23].
Além disso, há uma busca por um rosto mais fino com preservação do triângulo invertido da juventude, por meio da excisão da bola de Bichat, lipoaspiração facial e lipólise injetável. A aparência arredondada nos ângulos pode ser ainda mais reduzida com a aplicação de toxina botulínica no masseter. Nesse sentido, um estudo com 40 pacientes de rosto arredondado foi analisado e tratado por cirurgia de escultura facial, que incluiu pelo menos dois dos procedimentos combinados. Os procedimentos incluíram lipoaspiração facial, excisão da bola de Bichat, aumento do mento, aumento malar e lipólise injetável. As expectativas estéticas dos pacientes foram atendidas em 39 casos. Uma combinação de procedimentos é necessária para proporcionar ao rosto um contorno atraente [24].
Além disso, Yang et al., 2019 [7] foi um estudo observacional retrospectivo com 312 pacientes (idade média de 53,3 anos), realizado em uma única clínica médica. Dos 312 pacientes (261 mulheres e 51 homens), 197 foram submetidos à lipoescultura cérvico-facial, 54 passaram por lipoescultura em outras regiões, e 61 foram tratados com lipoescultura da parte inferior da face. Pacientes com índice de teste de Illoz <20%, com excesso leve ou moderado de pele na parte inferior da face, são indicados para lipoescultura da parte inferior da face, e excesso leve ou moderado de pele na área submentoniana (de acordo com o teste do beliscão) é indicado para lipoescultura cervical.
Além disso, antes e durante a operação, o paciente foi instruído a fazer caretas, assobiar e sorrir. O volume da lipoescultura variou entre 30 mL e 100 mL. O fechamento da ferida no pós-operatório não foi realizado. A bandagem compressiva foi usada por 5 dias. Dos 312 pacientes, apenas três apresentaram resultados insatisfatórios. Nos resultados pós-operatórios, apenas dois pacientes apresentaram rugas e um paciente apresentou irregularidades no contorno facial. Os três pacientes foram tratados com enxerto de gordura microestruturada e obtiveram resultados satisfatórios após a segunda cirurgia.
Além disso, os pacientes submetidos à lipoescultura cérvico-facial apresentaram redução do “marionete wrinkle”, remoção do acúmulo perioral, contorno facial em V, linha da mandíbula definida, redução da papada, projeção visual do queixo e elevação cérvico-facial. Portanto, a lipoescultura cérvico-facial mostrou-se vantajosa em termos de segurança e eficácia.
Conclusão
De acordo com os principais estudos clínicos selecionados no presente estudo, a lipoescultura cérvico-facial demonstrou ser segura e eficaz. Em pacientes com perda de volume facial, a transferência de gordura de alta densidade com injeção facial de SVF-gel resultou em escores de melhoria significativamente mais altos e maior satisfação dos pacientes, sendo observada uma aparência estética melhorada/muito melhorada. Como análise de acompanhamento dos estudos, em uma média de seis meses após a conclusão, a maioria dos pacientes estava satisfeita com os resultados. Ainda assim, os resultados dos estudos mostraram que o nível de autoconfiança e a qualidade de vida relacionada à saúde mental podem ser significativamente melhorados após o tratamento com lipoenxertia facial.
Major clinical outcomes and analysis of the risk of bias of the advances in
cervicofacial liposculture: a systematic review
Júlio Leal Villela Garcia, Vanessa Rodrigues do Prado Garcia, Sandro Marcelo de Moraes Valente
Abstract
Introduction: In the context of liposculpture,
cervicofacial liposuction involves the application of
negative pressure through a hollow cannula in the
subcutaneous plane to gently avulse fat cells and
accurately sculpt unwanted fat deposits on the face and
neck. Furthermore, lipo contouring provides a versatile
tool in the facial surgeon’s arsenal to achieve the desired
facial profile. In 2020, approximately 15.5 million
cosmetic procedures were performed in the United
States alone. Objective: A systematic review was
carried out on the main clinical results, presenting
studies on the risk of bias, and the advances in facial
and cervical liposculpture as an important aesthetic tool
for the dental surgeon. Methods: The rules of the
Systematic Review-PRISMA Platform were followed. The
search was carried out from November 2021 to February
2022 in Scopus, PubMed, Science Direct, Scielo, and
Google Scholar databases. Results: 64 articles were
found involving liposculpture. A total of 32 articles were
fully evaluated and 14 were included and developed in
the present study. Considering the Cochrane tool for risk
of bias, the overall assessment did not result in
significant risk of bias studies. The Funnel Plot showed
symmetrical behavior. Twenty-five studies did not meet
the GRADE. Most patients who were involved in the
studies showed improvements in facial augmentation
and contouring. In patients with loss of facial volume,
high-density fat transfer with the facial injection of SVFgel resulted in significantly higher improvement scores
and better patient satisfaction. Conclusion: According
to the main clinical studies selected in the present study,
cervicofacial liposculpture proved to be safe and
effective. In patients with loss of facial volume, highdensity fat transfer with a facial injection of SVF-gel
resulted in significantly higher improvement scores and
better patient satisfaction. Still, the results of the studies showed that the level of self-confidence and mental
health-related quality of life can be significantly
improved after facial lipofilling treatment.
Keywords: Liposculpture. Fat grafting. Lipo contour.
Facial liposculpture. Cervical liposculpture. Aesthetics.
Clinical trials.
Introduction
In the context of liposculpture, cervicofacial
liposuction involves the application of negative pressure
through a hollow cannula in the subcutaneous plane to
gently avulsion fat cells and accurately sculpt unwanted
fat deposits on the face and neck. Furthermore, lipo
contouring provides a versatile tool in the facial
surgeon’s arsenal to achieve the desired facial profile
[1-3]. In 2020, approximately 15.5 million cosmetic
procedures were performed in the United States.
Minimally invasive techniques that allow for faster
recovery are especially in demand. According to The
Aesthetic Society’s 2018 report, liposuction is the
second most popular cosmetic procedure in the United
States [1].
Also, in recent decades, improvements have been
observed in the techniques of suspending the superficial
musculoaponeurotic system and adjacent fat pads.
Thus, liposculpture (LS) can complement cervicofacial
aging surgery [2,3]. Minimally invasive procedures in
facial liposculpture are expanding and the transfer of
adipose tissue can result in ideal esthetic effects [3-5].
Thus, current liposuction techniques have evolved
over the years. Initially, direct excision of unsightly fat
pads as described in combination with superficial
musculoaponeurotic system (SMAS) facelift. Fat can be
removed through submental and post-auricular
rhytidectomy incisions, or excess ptotic fat and skin can
be excised directly from the jowls and dewlap. However,
as it is technically challenging to remove subcutaneous
fat deposits evenly with open techniques, these
attempts often produce uneven skin contours.
In this regard, lipo contouring techniques provide
a means to shape the neck and face fat deposits to
better obtain the desired facial profile [6]. The resulting
overall improvement has direct and indirect effects on
facial esthetics. For example, submental liposuction
produces a more pleasant acute cervicomental angle
and, at the same time, gives the illusion of greater
projection of the chin [7].
In this sense, historically, direct excision of skin
and fat led to long visible scars that were predisposed
to central depression and postoperative dog-ear
formation. Given the often unsatisfactory results
obtained with direct excision of fat, it was not
uncommon for surgeons to ignore the accumulations of
preparation, nasolabial, submental, and cervical fat, in
many cases producing a marked discrepancy in the
rejuvenated appearance of the upper face compared to
the face. lower and neck [8].
In this context, during the last decades, the
introduction of refined liposuction techniques, in
addition to platysma plication and surgical tightening of
the excess neck skin, gave the facial plastic surgeon the
ability to improve the contour of the jaw and definition
of the cervicomental angle. The versatility of the
liposculpture procedure, used alone or in combination
with rhytidectomy, malar and chin implants,
mentoplasty and other adjuvant procedures of facial
plastic surgery, combined with its excellent results, with
only small cosmetically hidden scars, technical ease and
minimal morbidity and recovery, popularized its use [7].
Thus, dental surgeons began to apply these
principles to the neck and jowls for facial rejuvenation
through minimal access incisions, including endoscopic
ultrasonographic lipectomy and the use of liposhavers.
Facial EL focuses on repositioning adipose tissue and
increasing facial transition zones. This is accomplished
by employing internal suspension sutures, as well as
with autologous fat grafting [6]. Therefore, LS is an
alternative to facial rejuvenation that involves the skin,
release of the retaining ligaments, and appropriate
removal of adipose tissue from the subcutaneous layer,
while improving skin tone and facial contour.
Also, a study presented experiences with 312
patients who underwent cervicofacial rejuvenation,
demonstrating the benefits of liposculpture in
cervicofacial rejuvenation in terms of reducing
marionette wrinkles, perioral mound removal, V-shaped
facial contour, defined jaw, reduced double chin,
protrusion chin visual, and cervicofacial lift [7]. Thus,
liposuction was a watershed in the evolution of cervicofacial LS, allowing the permanent removal of
excess adipose tissue located under the skin. Also,
several therapeutic means are in constant
improvement, such as the use of cutting cannula
followed by blunt cannula, laser/ultrasound-assisted
liposuction, as well as rotating and vibrating cannula
[8].
Therefore, the present study aimed to carry out a
systematic review of the main clinical results, presenting
studies of the risk of bias, and the advances of facial and
cervical liposculpture as an important aesthetic tool for
the dental surgeon.
Methods
Study Design
The rules of the Systematic Review-PRISMA
Platform (Transparent reporting of systematic reviews
and meta-analysis-HTTP://www.prismastatement.org/) were followed.
Data Sources And Research Strategy
The search strategies for this systematic review
were based on the keywords (MeSH Terms):
“Liposculpture. Fat grafting. Lipocontour. Liposculpture
face. Cervical liposculpture. Aesthetics. Clinical trials”.
The search was carried out from November 2021 to
March 2022 in Scopus, PubMed, Science Direct, Scielo,
and Google Scholar databases. In addition, a
combination of keywords with the Booleans “OR”, “AND”
and the “NOT” operator were used to target scientific
articles of interest.
Study Quality And Risk Of Bias
The quality of the studies was based on the GRADE
instrument [9] and the risk of bias was analyzed
according to the Cochrane instrument [10].
Results and discussion
Findings Summary
It was found 64 articles involving facial and cervical
liposculpture. Initially, article duplication was excluded.
After this process, the abstracts were evaluated and a
new exclusion was performed, removing the articles
that did not include the topic of this article. A total of 32
articles were fully evaluated and 14 clinical studies were
included and developed in the systematic review.
Twenty-five studies did not meet the GRADE (Figure
1). Considering the Cochrane tool for risk of bias, the
overall assessment did not result in significant risk of
bias studies (Figure 2).
Figure 1. Article selection (Systematic Review, N=14
clinical studies).
Figure 2 presents the results of the risk of bias in
the studies using the Funnel Plot, through the
calculation of the Effect Size (Cohen’s Test). The sample
size was determined indirectly by the inverse of the
standard error (1/Standard Error). The graph showed
symmetrical behavior, not suggesting a significant risk
of bias in the studies with small sample sizes that are
shown at the bottom of the graph.
Figure 2. The symmetrical Funnel Plot does not suggest a risk of bias between the small sample size studies that
are shown at the bottom of the graph.
Figure 3 presents three illustrative images, where
images A and B represent the positioning and
penetration of the cannula for liposuction, and image C
represents the result of the reduction of adipose tissue
in the highlighted region. The images belong to a patient
(with confidential information, without presenting the
clinical case) of the authors of the present study, in
order to exemplify the liposculpture procedure, as well
as to demonstrate that the procedure can be performed
safely.
Genetic, Epigenetic, and Pathophysiological
Aspects as Predictors for Liposculpture
The cervicofacial characteristics of each individual
are determined by the underlying bone and cartilaginous
structure and the coverage of the skin and soft tissue
envelope. These characteristics are all determined at the
genetic level but can be influenced to varying degrees
by environmental factors (epigenetics) such as nutrition,
exercise, aging, medications, exposure to toxins, actinic
damage, trauma, and surgery [11,12].
As adverse epigenetic factors exert their impact,
ptosis of the facial support structures causes the malar
and buccal fat pads to fall. The loss of skin elasticity
produces thick and thin wrinkles and sagging of the
facial skin. Tissue laxity and maldistribution of fat
deposits lead to the formation of double chin and
dewlap, redundant loose tissue hanging over the
mandible and chin, respectively. In the neck, fat
accumulation and platysma ptosis result in prominent
bands producing a “turkey-eater” appearance. Patients
with congenitally low hyoid bones have a more
compromised definition of the cervicomental angle [12].
Figure 3. Three illustrative images, where images A and B represent the positioning and penetration of the cannula
for liposuction, and image C represents the result of the reduction of adipose tissue in the highlighted region.
Source: Own author.
Furthermore, the loss of fat on facial was
emphasized as a component of aging [12-14]. Volume
reduction, particularly in the periorbital, cheek, and
perioral areas, plays a prominent role in creating a facial
cavity and skin laxity. Removal of body fat from sites
and subsequent reinjection into areas of atrophy is ideal
[15-18]. Fat viability is influenced by several factors,
including harvesting method, cleaning, particle size, and
reinjection cannula size. Minimizing vacuum extraction
pressure causes less immediate cell trauma. The
smallest cannulas should match the injection cannula to
minimize transfer compression. Cleaning can be carried
out by rinsing or centrifuging. Smaller pieces of adipose
tissue are recommended to minimize lumps and
increase surface area [19].
In this context, it is noteworthy that the most
common areas of fat injection are the cheeks and
nasolabial folds, where the tissue is thicker and muscle
movements are minimal. Periorbital injections are
another option, but very fine particles are needed to
prevent lumps from forming. The perioral area and lips
are the least predictable in retention, presumably
because of underlying muscle movement [7].
Also, some young individuals have a genetic
propensity for undesirable facial fat distribution despite
normal body weight. For example, the baby’s submental
accumulation of fat can persist into adulthood. These
patients usually have excellent skin and muscle tone and
may benefit only from selectively closed liposuction. Fat
accumulation in adulthood can occur due to adipocyte
hyperplasia and not cell division. Liposuction reduces
the total number of adipocytes by directly removing cells
and inducing localized apoptosis as a result of
mechanical trauma and devascularization. Adipocytes
that remain after LS are a stable population and are not
more prone to hyperplasia than are adipocytes
elsewhere in the body. Thus, the improvement of the
facial profile after liposuction is maintained as long as
there is no generalized excessive weight gain [3].
Major Postoperative Care
Postoperative management is divided into theimmediate postoperative period (the first 24 hours) and
the subsequent period. Immediate postoperative care
focuses on preventing hematoma through blood
pressure control. Again, for practical purposes, the
systolic blood pressure level is more indicative than the
diastolic one. Maintenance of a postoperative systolic
pressure of less than 140 mm Hg is desirable [20].
Intraoperative treatment with a 0.1 to 0.2 mg
clonidine transdermal patch often attenuates injectionassociated hypertension and subsequently the
absorption of epinephrine into the local anesthetic
solution. In patients who are not on blood pressure
medication (particularly beta-blockers), intraoperative
hypertension can be controlled with 5 to 10 mg boluses
of labetalol. It is important to avoid adding additional
beta-blockers in patients who are already beta-blocked
and showing relative bradycardia. Within such patients,
0.25 mg bolus of calcium channel blockers such as
nicardipine can be administered intraoperatively.
Adrenaline injected from the local anesthetic solution is
slowly absorbed, so post-operative bruising usually
occurs four to 10 hours after surgery. Postoperatively,
labetalol can be administered orally in doses of 100 mg.
Alternatively, a pure alpha agonist (such as 0.1 to 0.3
mg clonidine) can be administered orally [21].
Also, prolonged post-operative swelling can cause
facial skin relaxation stress and lead to a compromised
outcome. The degree of postoperative edema is related
to the extent of the dissection, not the depth. Limited
salt intake (preferably 1000 mg/day) and reduced fluid
intake may also be beneficial. The potential value of
perioperative corticosteroids remains controversial.
While craniomaxillofacial surgeons felt it was beneficial,
199,200 others found no benefit for facelift swelling
[20,21].
Major Complications [3]
✓ Hematoma
✓ Skin Necrosis
✓ Infection
✓ Nerve Injury
✓ Fibrosis
✓ Deformities (hypotrophy or hypertrophy)
Major Clinical Studies – Systematic Review
Analysis (N=14 clinical studies)
In the context of lipofilling and liposculpture,
treatment to improve skin characteristics related to
aging such as wrinkles, pigmentation spots, pores, or
rosacea has become a practice to improve the health of
the skin and the whole organism, as this positively
impacts the quality of the skin. patients’ lives. In this
sense, optimizations are being carried out. Thus,
different additives such as platelet-rich plasma (PRP) or
stromal vascular fraction (SVF) have been combined
with lipofilling to increase the therapeutic effect and
stability of adipose tissue-derived stromal cells (ASCs).
For this purpose, a randomized, prospective, doubleblind, placebo-controlled study examined the hypothesis
that mechanically isolated SVF enhances the therapeutic
effect of lipofilling supplemented with PRP to improve
facial skin quality. In total, 28 women were enrolled; 25
completed follow-ups within 1 year of the postoperative
period. Compared with PRP-supplemented lipofilling,
PRP-supplemented lipofilling combined with SVF did not
improve facial skin quality or patient satisfaction in a
healthy population, but it was a safe procedure [22].
Furthermore, a study investigated the impact of an
aesthetic intervention on the self-perception of
improved facial appearance and quality of life (QoL)
after 1 and 6 months of follow-up. A total of 63
consecutive individuals undergoing facial lipofilling were
included in the study. There was a statistically significant
improvement in QoL at each subsequent time point,
compared to baseline, across the SF-36 domains, except
for the physical functioning and pain subscales. It is
noteworthy that advanced social life was strongly
associated with improved satisfaction with facial
appearance, better self-esteem, and lower levels of
anxiety and depression during the follow-up period after
facial lipofilling. The results of this study supported the
hypothesis that the level of self-confidence and mental
health-related quality of life can be significantly
improved after facial lipofilling treatment [23].
Also, there is a quest for a slimmer face with
preservation of the inverted triangle of youth with buccal
fat pad excision, facial liposuction, and injection
lipolysis. The rounded appearance at the angles can be
further reduced by injecting botulinum toxin into the
masseter. In this regard, a study of 40 patients with
round faces was analyzed and treated by facial sculpting
surgery, which included at least two of the combined
procedures. Procedures included facial liposuction,
buccal fat pad excision, chin augmentation, malar
augmentation, and injection lipolysis. Patients’ aesthetic
expectations were met in 39 cases. A combination of
procedures is required to give the face an attractive
contour [24].
Besides, Yang et al., 2019 [7] that was an
observational retrospective with 312 patients (mean age
53.3 years) that was performed in a single medical clinic.
Of the 312 patients (261 women and 51 men), 197
underwent cervicofacial liposculpture, 54 underwent
liposculpture of other regions, and 61 were treated with
liposculpture of the lower face. Patients who had an Illoz
test index <20%, with mild or moderate excess skin on
the lower face, are recommended liposculpture of the
lower face, and light or moderate excess skin in the
submental area (according to the pinch test) is
suggested for cervical liposculpture. Also, before and
during the operation the patient was obliged to grimace,
whistle and smile. The volume of liposculpture was
between 30 mL and 100 mL. Postoperative wound
closure was not performed. The compression band was
used for 5 days. Of the 312 patients, only three had
unsatisfactory results. In the postoperative results, only
two patients had wrinkles and one patient had facial
contour irregularities. The three patients were rescued
with a micro fat graft and achieved satisfactory results
after the second operation. Also, patients who
underwent cervicofacial liposculpture showed reduced
wrinkle puppet, perioral mound removal, V-shaped
facial contour, defined jawline, double chin reduction,
visual chin protrusion, and cervicofacial elevation.
Therefore, cervicofacial liposculpture proved to be
advantageous, in safety and efficacy.
Furthermore, a study with 210 patients evaluated
the aesthetic results and patient satisfaction after
bimaxillary orthognathic surgery with or without
simultaneous facial lipofilling procedures. A patient
questionnaire was used to assess perceived
improvement in esthetics. One hundred and twenty
patients (mean age 20.3 years) underwent bimaxillary
orthognathic surgery and simultaneous facial lipofilling
procedures (group I). The remaining 90 patients (mean
age 19.8 years) underwent skeletal procedures only
(group II). The overall esthetic improvement was similar
in both groups (group I 92.5%, group II 91.1%). Higher
higher-level esthetic improvement scores were recorded
for group I (group I 80%, group II 55.6%). Overall
patient satisfaction was 98.3% for group I and 97.8%
for group II. Higher-level satisfaction scores were
recorded for group I (group I 14.2%, group II 6.7%).
The simultaneous use of autologous fat micrograft is a
promising technique that can improve the aesthetic
results of orthognathic surgery, leading to greater
patient satisfaction [25].
In addition, autologous fat grafting targeted at the
LS process is commonly used for soft tissue
augmentation and reconstruction, however, it is limited
by a high graft absorption rate. Stromal vascular fraction
gel graft/Stromal vascular fraction (SVF-gel) for facial
volume augmentation may have a positive effect on skin
rejuvenation, however, its major limitation is the low
conversion rate of Coleman’s fat. In this regard, one
study investigated a new surgery using high-density fat
in combination with SVF-gel in the treatment of
hemifacial atrophy or Romberg’s disease. From October
2017 to October 2019, 13 patients with hemifacial
atrophy underwent high-density fat transfer with SVFgel injection. The result was determined by the
difference in the pre and postoperative FACE-Q modules
(FACE-Q conceptual structure: 1, Satisfaction with Facial
Appearance; 2, Health-Related Quality of Life; 3,
Negative Sequelae; 4, Satisfaction with the Care
Process). Cosmetic results were observed during followup periods, with no adverse events observed in the
treatment group. All patients showed improvements in
facial augmentation and contouring. In patients with
loss of facial volume, high-density fat transfer with a
facial injection of SVF-gel resulted in significantly higher
improvement scores and better patient satisfaction. The
preoperative and postoperative results of the FACE-Q
modules reported by the patient showed statistically
significant improvement [26].
Furthermore, a prospective controlled study
evaluated the 6-month contouring efficacy of 1470
radial fiber-assisted liposuction and the effect of a
volumetric increase of tissue harvested in facial fat
grafting. Twenty individuals underwent lower abdominal
or external thigh liposuction. In seven individuals,
samples were grafted onto facial regions. Treatment
safety, body weight, esthetic improvements rated by the
blinded evaluator, and subject-rated satisfaction were
monitored for 6 months. Abdominal and facial fat
thickness was assessed by magnetic resonance imaging
(n=5) within 3 months of treatment. One month after
treatment, most subjects rated improvements as
good/excellent (88%) and skin tightening
satisfactory/very satisfactory (92%), with over 70% of
subjects providing similar scores 6 months after
treatment. Improved/much improved aesthetic
appearance (87%) was observed. Harvested tissue
injected as a facial filler (21.0 ± 5.2 ml) led to a 0.63 ±
0.12 mm increase in facial fat thickness, as observed by
MRI, at 3 months. Six months after completion, most
subjects (83%) were satisfied with the result. All
procedures were well tolerated [27].
Despite this, several problems such as facial
lipodystrophy and changes in the skin and skin texture
have not yet been fully resolved. Thus, a retrospective
observational clinical study analyzed the use of the LipoFacelift procedure, which consists of facial liposculpture
performed simultaneously with a bivector biplanar
facelift procedure of the submucosal aponeurotic
system. The authors analyzed pre-and post-surgical
photographs of 12 Lipo-Facelift patients after 3 and 12
months and analyzed their medical records for
complications. In addition, CO2 measurement was
performed to assess the improvement of
microcirculation. The longest follow-up period was 8
years. The Lipo-Facelift demonstrated very satisfactory
results and no surgical intervention or revision was
required. The results showed a lasting improvement in
skin quality [28].
In the previous study, the results can be achieved
due to the improvement of angiogenesis due to the
growth factors transferred in the lipoaspirate, as well as
in the presence of adipose mesenchymal stem cells, and
exosomes, microRNA, and pericytes. Furthermore, the
differentiation of progenitor cells into fibroblasts and
increased collagen production contribute to firmer skin
[29]. In particular, Coleman’s lipo structure is a
procedure for transferring adipocytes, based on rigorous
methodology and the use of specific material [30].
In this sense, a retrospective study involved 100
patients who underwent volumetric facial restoration
with facelift and liposculpture. The mean surgery time
was 15 months. Overall patient satisfaction was 82%
with a mean score of 15/20 in the subjective assessment
and 13.3/20 in the objective assessment. The results
differed significantly according to the facial aesthetic
subunit involved, with the best results being obtained in
the malar region and cheek, and the least satisfactory in
the upper and lower lips. Prolonged edema was the only
complication (8%) [31].
Furthermore, a prospective clinical study described
the surgical results with special emphasis on
complications in patients undergoing high-definition
liposculpture. A total of 417 patients underwent highdefinition liposculpture between 2015 and 2018. Primary
liposuction and secondary liposuction were performed in
308 (74%) and 109 (26%), respectively. Combined
surgeries were performed in 121 cases (29%). There
were no systemic complications. Local complications
included hyperpigmentation (n=276), seroma (n=125),
nodular fibrosis (n=83), unsatisfactory definition in the
areas of superficial liposuction (n=16), unnatural
appearance of the body contour (n=17), VASER-related
burns (n=3) and Mondor syndrome (n=2). Most patients
(94%) were satisfied with the results [32].
Also, a retrospective clinical study demonstrated
that a spectrum of liposculpture definitions can be
achieved using Power-Assisted Liposculpture (PAL)
liposuction. The authors described satisfaction and
complication rates. Fifty male patients were included in
this study between January 2018 and November 2019.
The mean age was 37.34 years. The mean body mass
index was 26.4 kg/m2. A total of 54.3% of patients
opted for the high definition (HD), 36.4% for the
moderate definition, and 9.2% for the light definition.
There were no major complications. The HD subgroup
had the highest incidence of minor complications (21%).
Patient satisfaction levels were high in all 3 subgroups,
with the highest scores in the HD subgroup (9.3/10) [5].
Finally, efforts to achieve predictable skin
retraction have largely neglected the importance of the
adipose tissue removal mechanism, focusing instead on
the depth of the surgical plane and the vacuum pressure
used. Recent experimental and clinical evidence points
to the role of mechanical displacement as a key factor
in the removal of adipose tissue. Thus, a modification of
an existing cannula design was used to achieve
predictable skin retraction on the face and neck in a
series of 75 patients with a 3-month to 3-year followup. Elevation of the facial and cervical flap with this
instrument (with or without deep tissue tightening and
skin excision) showed consistently improved results,
improving skin tone and facial contours while decreasing
recovery and operative time. The combination of the
described technique and existing techniques such as
endoscopic and compound lifting approaches can
improve the achievable results [33].
Conclusion
According to the main clinical studies selected in
the present study, cervicofacial liposculpture proved to
be safe and effective. In patients with loss of facial
volume, high-density fat transfer with SVF-gel facial
injection resulted in significantly higher improvement
scores and better patient satisfaction, with an
improved/much improved esthetic appearance being
observed. As a follow-up analysis of the studies, at an
average of six months after completion, most patients
were satisfied with the results. Still, the results of the
studies showed that the level of self-confidence and
mental health-related quality of life can be significantly
improved after facial lipofilling treatment.


